Talk: Transforming health and delivering the NHS 10-year plan
Slides and speaker notes from a talk about the NHS 10-year plan
In September, I was asked to give some thoughts about the NHS 10-year plan based on the principles in Platformland. Here are the slides and speaker notes.
Platformland makes the case for public services that work much harder for the public and public servants, where design and delivery are radically simpler, faster, and cheaper, and the system engages the public as co-producers, not mere consumers.
What follows are some thoughts on applying some of those principles in the context of the NHS in England and the ambition of the 10 year plan.
Firstly, the shift from analogue to digital that the 10-year plan calls for is about more than applying digital technology. It's about applying digital ways of working.
As James Plunkett has said, when people hear the word ‘digital’, they still think we’re talking about technology. That or it’s used as shorthand for efficiency or some abstract concept of 'innovation'.
But in years to come, we’ll look back and realise that the most significant impact of digital for the work of the public sector was not technology it was organisational. That’s because digital practice opens up a new way of working and running organisations. The model of iterative delivery may have first emerged as a way of building software, but it has since proven far more broadly applicable as a way of approaching complex problems.
Digital-era ways of working are highly responsive, capable of learning, and making progressive improvements, and rapidly scaling.
One example of this non-digital application of digital ways of working was something I was involved in when I was a civil servant: Universal Credit. After the initial failure of the project, it was launched in a single postcode district in Sutton with a tightly focused team, scaling when the team had confidence to do so. They were also able to chase down indicators like the number of claims paid on time.
The model is clear: empower teams to think big, start small, scale what works. This is not about publishing more strategy docs with key metrics, about creating teams with the dynamic capability to deliver what’s needed most.
The reason the model is powerful is that - rather than fixing scope upfront - teams can operate within rapid feedback loops - spotting a problem, trying something, learning, and progressively improving, and then scaling those improvements across the system.
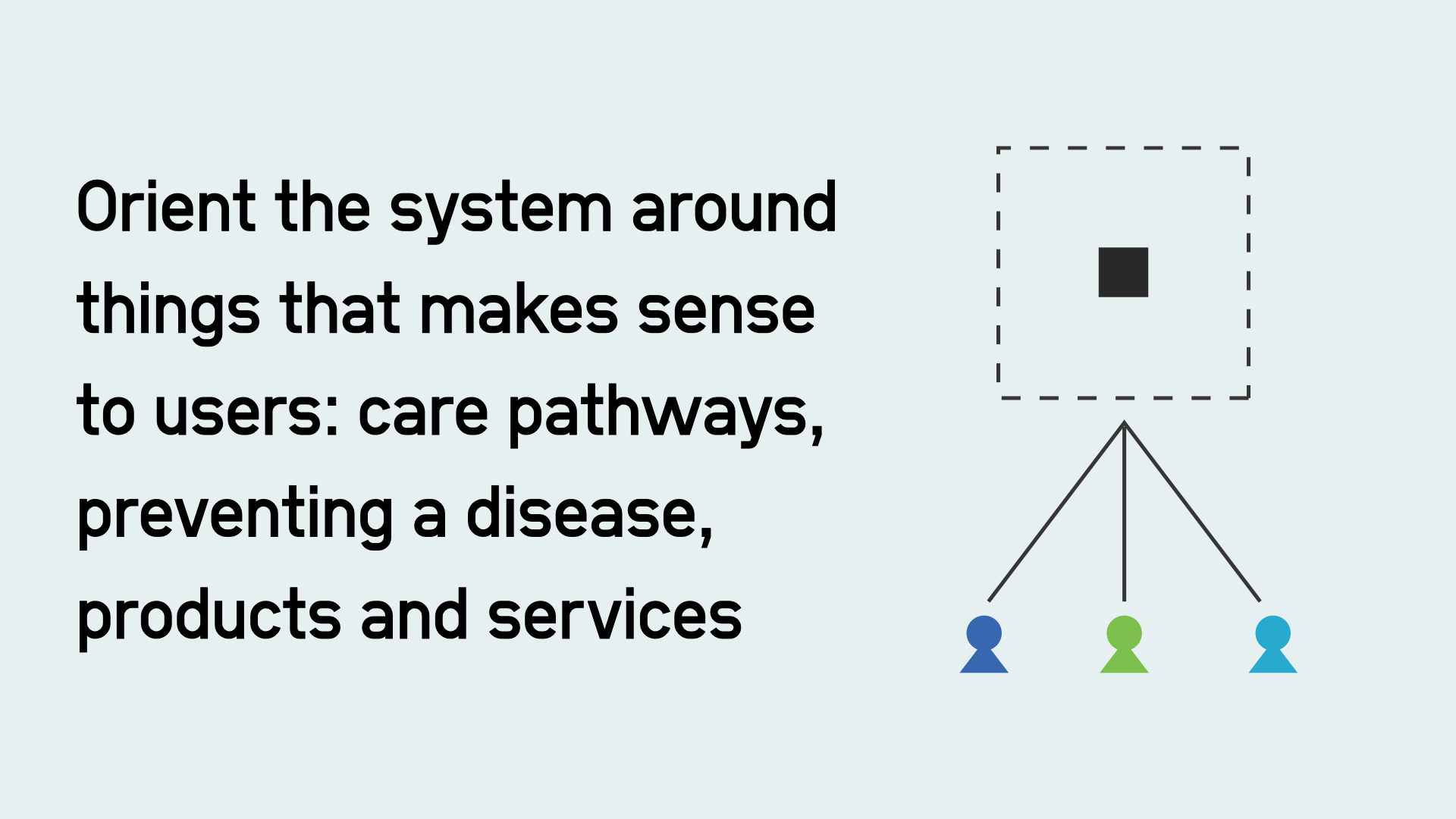
Digital organisations also organise their work around things that make sense to users. Amazon doesn’t have separate apps for different towns or types of goods. They organise around products and services like Kindle, online shopping, and Alexa. They do this so things work for those users and achieve the organisation’s goals.
The application of digital to the public sector is partly the reorganisation of the work of the public sector around different things.
In the NHS, that means, rather than organising things by settings like primary and secondary care a digital era NHS needs to organise more of the system’s key teams and institutions around things that make sense to patients. So, products, like the NHS App. Simple platforms like NHS Notify. Services, like getting vaccinated. Care pathways, like cancer diagnosis and treatment.
Reorganising the work of the NHS won't happen just because there is a line in a spreadsheet saying something will be delivered. It takes leadership to choose where to place people, money and accountability.
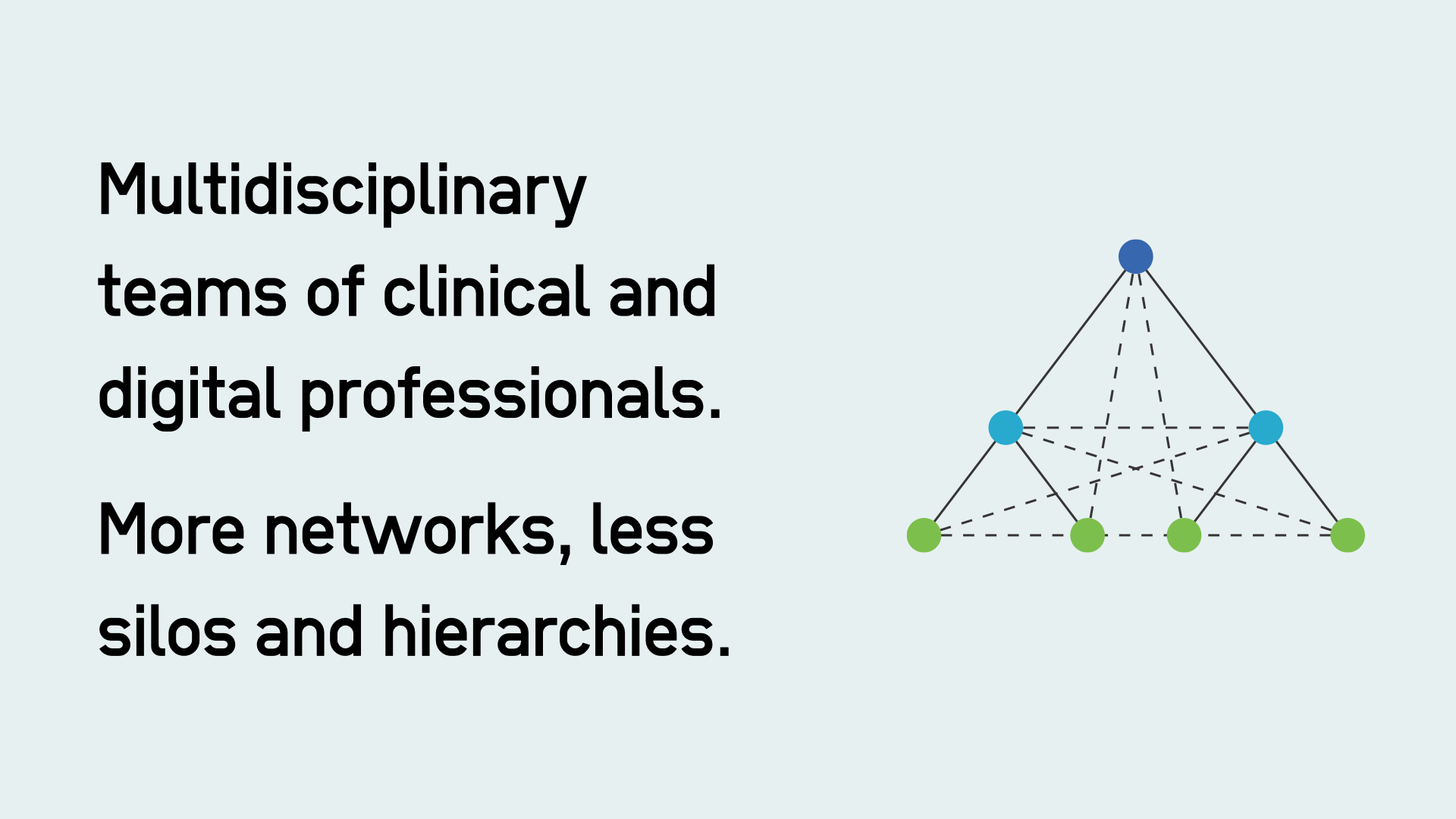
That means the NHS cannot continue to treat digital as a silo. Setting up these sorts of teams means moving away from functional silos and hierarchical governance to multifunctional teams with digital, clinical, and public health professionals working on the same teams to achieve the same outcomes, wherever they are needed in the system.
As an example of this in the real world, I met a team in Chile a few months ago from the LIP UC. They had created a multidisciplinary team of designers, researchers and nurses to successfully reduce waiting lists (some lists were nearly 8 years long). They did this mostly by identifying and scaling practices already existed, but were dispersed across several healthcare facilities.
The NHS could emulate this approach, creating a dozen or so multidisciplinary teams focused on outcomes, e.g. reducing diabetes, designing a digital-first GP surgery, or eliminating health admin for cancer patients. It could start creating more of those teams today.
This will also require the NHS to work as in a much more networked way. Leaders creating an expectation of collaborative open working that allows teams to learn from each other.
This, in turn, will need people with genuine experience of working as part of digital delivery teams at the most senior levels across the system.
As well as wider adoption of digital ways of working, the NHS needs to apply digital platform thinking to everything it does.
There is already a lot of duplication, fragmentation and a lack of standards in the system, with hundreds of CRMs, appointment systems and patient record systems. The move to neighbourhood health, virtual hospitals, and greater autonomy for integrated health organisations, risk compounding the problem. It even risks the delivery of parts of the 10 year plan, if they get wrapped up in the inertia of procuring multiple systems.
Rather than treating technologies like buildings, as if everyone needs their own one, common platforms can be provided once and used many times.
Platform thinking isn't some sort of spreadsheet exercise where an organisation picks a 'target architecture', or picking monolithic systems that claim to do everything off the shelf, but in reality spawn busywork for consultancies customising them.
Platforms also blur the line between ‘central vs local’. Centrally provided platforms can enable local delivery. So we should beware of any conversation that simplistically talk about moving capacity to one part of the hierarchy, It just doesn’t make sense in the digital age.
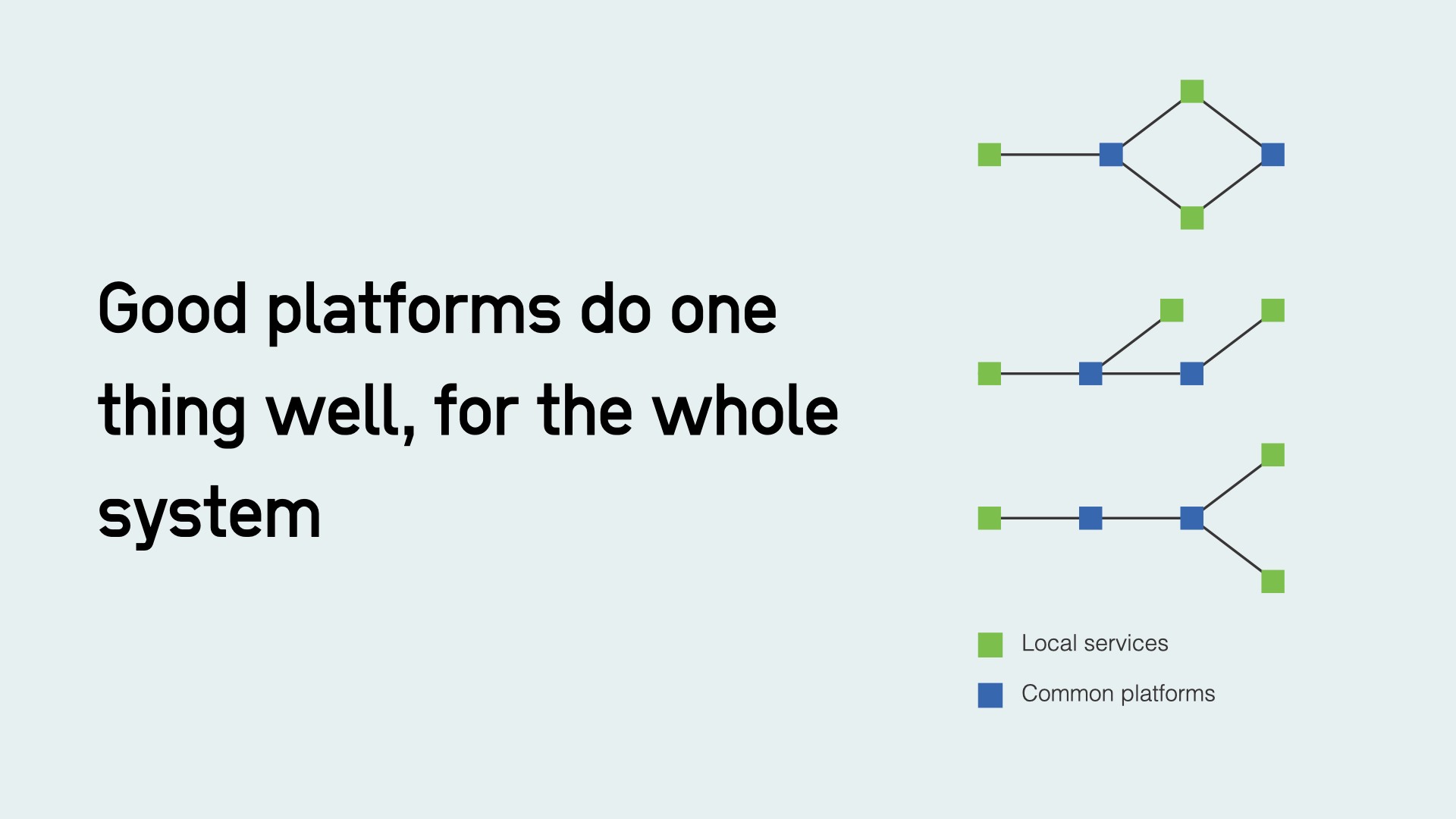
Good platforms do one thing well, for the whole system. They are products designed to meet the needs of users (mostly staff), enable local innovation and, with scale, bring lower costs.
Obviously, the NHS already does this with things like prescriptions in the app , Cohort as a Service, or Record a Vaccination. But it needs to do more, which I’ll come onto in a minute, but today it mostly it leaves the system to fend for itself.
Platform thinking is not purely about reducing the costs of duplication either. The unseen costs of back-office systems that don’t work for clinicians and the public often dwarf any cost of duplication.
According the the Kings fund, nearly two in three patients and carers had experienced an admin problem in the last year. Four in ten of those say they are less likely to seek care in the future. It effects care and admin and clinical staff bare the brunt of the public frustration. Digital Public Infrastructure can help provide a better service to the public by meeting the needs of staff.
Today, the NHS relies too much on mandates to get the system to adopt technology. As Ben Welby puts it, mandates solve adoption but they don’t guarantee success.
Successful Digital Public Infrastructure should aim to be so good it’s negligent not to use it.
This is what India did when it launched the platforms for its health mission. The Unified Health Interface has linked 739 million health records, without hard mandates. That number was about half that of the previous year. It was launched in some areas before scaling. What if the NHS tried that with the single patient record? Starting small with one area?
To create platforms that meet the needs of frontline teams and providers, the NHS needs to do the work to understand what they really need, not on paper, but in reality by conducting research with them. That was how GDS identified the need for GOV.UK Forms, for example. Collecting information was the top need that service teams had.
Many of the common needs that neighbourhoods and trusts have will not be things we might typically think of as digital. Many may be clinical. Things like digital phlebotomy and home testing fulfilment, or questionnaires for common checks or assessments like the mental health monitoring. Starting today, the NHS could commission the work to identify the ten most common tests, questionnaires, or referrals that neighbourhood health teams need, and create easy-to-use options for local teams.
Pivoting the NHS to prevention requires treating the public as co-producers of health outcomes, not as consumers of a service.
It’s trivial to use technology to tell someone to stop smoking or lose weight, but hard to get people to do something about it. And to do something that works.
This is a challenge for the NHS, but also for contemporary digital practice in the UK public sector, which has a utilitarian outlook, with the aim to get people to 'done' as quickly as possible.
Luckily, digital may give us some new ways to co-produce health outcomes if we think about the design of NHS product in the right way.
For example, the NHS app could make it possible for clinicians to collect Patient Reported Outcomes for any given intervention.
Today, I think I’m right in saying that the NHS only collects Patient Reported Outcomes for two interventions: knee and hip surgery.
As Simon Wardley has pointed out, its hard to imagine how you train AI for some of the more speculative healthcare use cases without those data points.
The NHS app and the work to create a 'single patient record' could make outcomes a first-class citizen in a patient's and a clinician's experience.
Measuring outcomes will be important for preventative referrals and social prescribing for things like weight management. It will be important to know if a particular weight management provider in, for example, Woking or Burnley, is making a difference.

Neighbourhood delivery of prevention risks fragmentation and a lack of coherence. The mess of every local authority maintaining a ‘local offer’ website for SEND children, which each cost local authorities money and are too often awful to use, is something to avoid. Treating digital services like physical goods to be purchased geography by geography rarely makes ends up making sense to users (or anyone but software vendors, for that matter).
However, because digital blurs the boundaries between central and local, national products like the NHS app can be designed with 'curated slots' for local delivery, giving local services national reach, and certainty and consistency of user experience for users, all while preserving local decision making.
We need to avoid tempting but oversimplistic models like 'marketplaces' or 'service catalogues'. The opportunity is to design national services like the NHS app to support long-lived relationships bwteen the public, their health and clinicians.
Good design, better data, AI and automation mean we can start to design more services that look like this …
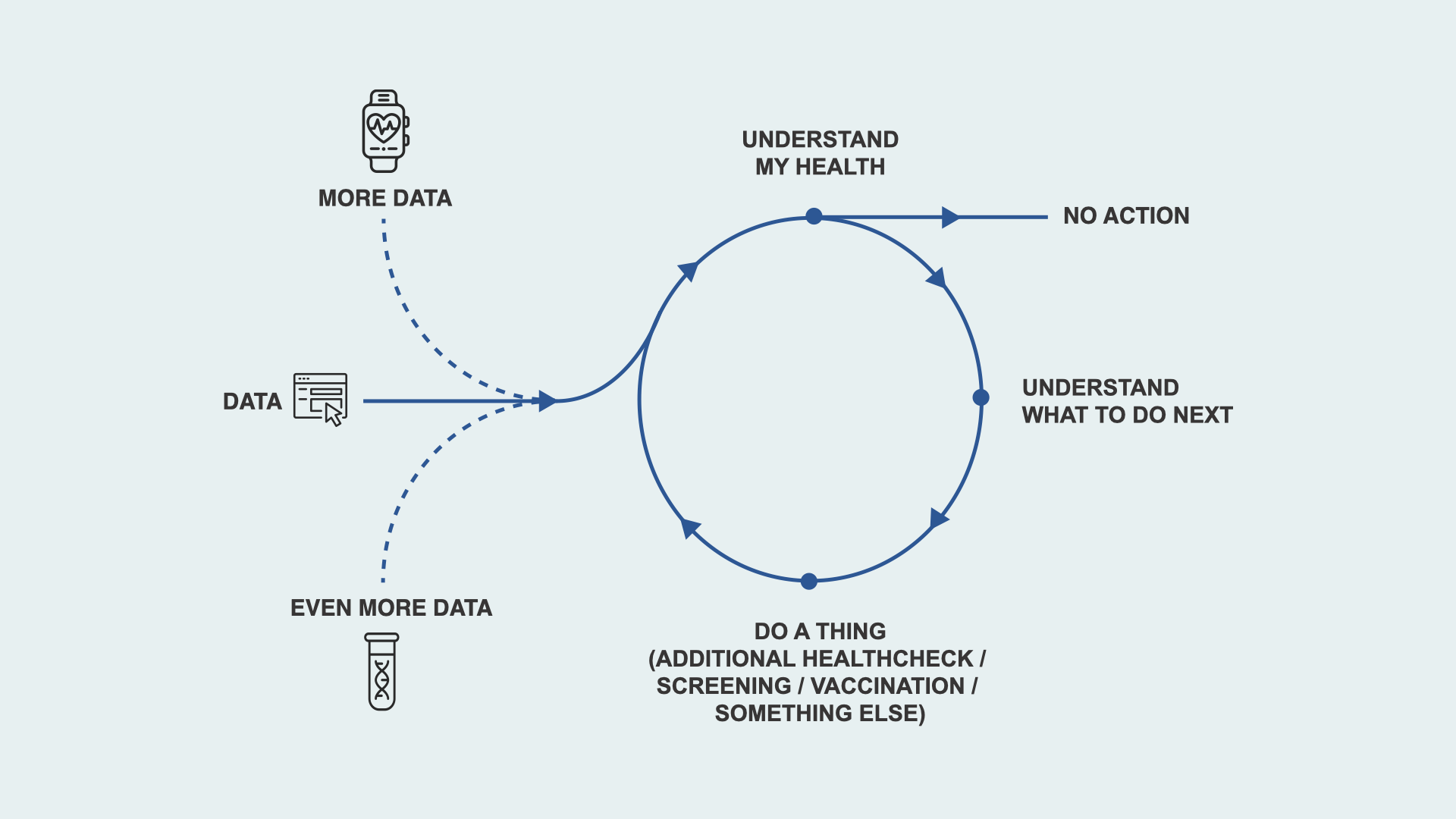
Services where there is an ongoing loop where patients can understand their health, understand what to do next, and are then supported to do it. Each loop creates more data.
Those are not primarily technology or data problems, they are clinical and interaction design questions. You need to understand what works, what can be automated, and what cannot before you attempt to scale.
We should not mistake things like AI health coaches or chat as technology purchases. Circling back to the bringing of my talk, we only find out what works by trying to go around this loop for real.
Organising to test assumptions probably means a lot of hand-cranking in the short term, just as when Universal Credit launched it had a digital interface, but much of the behind the scenes processes were still manual.
Starting to create those feedback loops does not have to be expensive, but it does require a certain mindset.

Finally, the NHS needs to start thinking like a tech company - but not in the way people normally think about that cliché.
The NHS has to manage two very different 'markets' at the same time: GP and hospital IT, and on the other hand, big tech companies in the form of things like Apple Health and others who will want to own the relationship with the public and have privileged access to data entered via their services.
Modern digital organisations use a mix of strategies to operate effectively in digital markets, markets which tend towards monopolies. They place themselves at critical infrastructure choke points, ensure they control the user interface, and use source code and standards as strategic tools.
That’s why Android’s open source - it was a moat strategy for Google’s search business. It’s, allegedly, why Facebook knew to buy WhatsApp. It’s how the US government got disintermediated by Turbo Tax and every US tax payer had to use its software. And it’s why Apple is pushing for FHIR adoption for its health products.
Luckily, there are examples from the public sector where this is already happening. The NHS could emulate what MHGLG have done in local government by seed funding alternatives. Through the local digital fund, they have created competitors to back office planning software that are better for local government staff and have standards baked in.
That represents a very different model to publishing standards and mandates (which inevitably get little traction), it’s about setting standards and showing what's possible in code.
Rather than ask how we can get more Trusts using Electronic Patient Record systems, for example, the aim should be to use a mix of control points and open-source to leapfrog the current Electronic Patient Record paradigm. We should ask: what comes next?
There is an interesting lesson here from city government in India. Cities were reliant on big monolithic Enterprise Resource Planning systems. A project called DIGIT from the eGov foundation took the approach of providing a series of opensource micro services that helped cities simultaneously get off legacy software and modernise their architecture at the same time. DIGIT didn't just create an open-source Enterprise Resource Planning system, they created something new. In some states, the state government has paid for every city to have an instance. Could a Software as a Service version of an open-source Electronic Patient Record system be centrally hosted by the Department for Health and Social Care, or a collection of NHS Trusts?
Another way to leapfrog the EPR paradigm is from the clinical side. In the same way an Uber passenger and Uber driver have their own version of the Uber app - what is there was a clinician app? They you suddenly you can start exerting pressure from both sides.
The NHS app already exerts market pressure because it mediates the relationship with the public, could a set of clinician-facing tools start to move some functions away from legacy systems?
It's at least worth considering.
In summary, I've talked about four things today:
- Digital ways of working, not just digital technology
- Apply platform thinking to clinical functions and understand local needs
- Convert the public from consumers to co-producers
- Proactively shape the software environment the NHS operates in
But if there's one common theme here, it's feedback loops.
Services that continuously improve reduce admin burdens for the public and staff, and save time and money.
A real-time understanding of what is working means you know what to scale when.
Teams providing national platforms are attuned with organisations across the NHS and so less reliant on mandates.
The public better understand their health, and clinicians better understand their patients.
And the NHS continues to understand and shape the shifting software environment it operates.